Research in the field of Adult ADHD is in rapid growth in Europe in these years, last fall Franke et al. made the review "ADHD: Live Fast, Die Young?" on ADHD across the life span and now an updated consensus on Adult ADHD has been released. We take a look at it here ...

Research in the field of Adult ADHD is in rapid growth in Europe in these years, last fall Franke et al. made the review “ADHD: Live Fast, Die Young?” on ADHD across the life span and now an updated consensus on Adult ADHD has been released. We take a look at it here …
Clinicians should also be aware that high functioning adults with ADHD may not present with a typical pattern of functional impairments in their daily life. Adaptive or compensatory skills can develop that mask the more overt behavioral problems related to ADHD.
(Kooij et al., 2019)
Attention-deficit/hyperactivity disorder (ADHD) is among the most common psychiatric disorders of childhood that often persists into adulthood and old age. Yet ADHD is currently underdiagnosed and undertreated in many European countries, leading to chronicity of symptoms and impairment, due to lack of, or ineffective treatment, and higher costs of illness (Kooij et al., 2010).
Besides information on the genetics and neurobiology of ADHD, three major questions are addressed in this statement:
(1) What is the clinical picture of ADHD in adults?
(2) How can ADHD in adults be properly diagnosed?
(3) How should ADHD in adults be effectively treated?
ADHD often presents as an impairing lifelong condition in adults, yet it is currently underdiagnosed and treated in many European countries, leading to ineffective treatment and higher costs of illness. Expertise in diagnostic assessment and treatment of ADHD in adults must increase in psychiatry. Instruments for screening and diagnosis of ADHD in adults are available and appropriate treatments exist, although more research is needed in this age group (Kooij et al., 2010).
There are two diagnostic manuals used to diagnose ADHD:
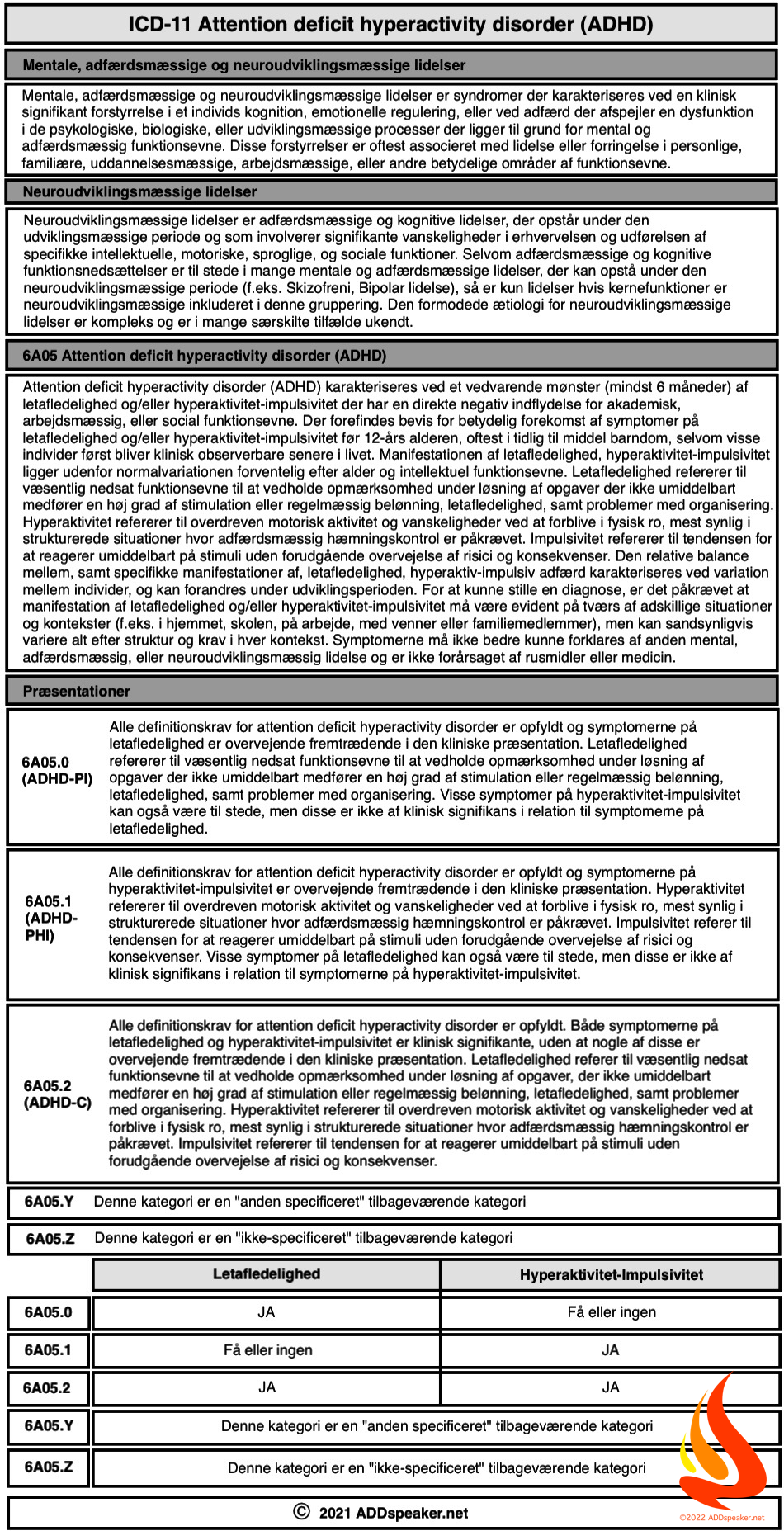
The Diagnostic and Statistical Manual of Mental Disorders (DSM) and the International Statistical Classification of Diseases and Related Health Problems (ICD).
As ADHD has been recognized as a disorder affecting individuals across the lifespan, the diagnostic criteria for adolescents and adults have been adjusted in the DSM-5, published in May 2013, and lastly in ICD-11 which was released in June 2018, for implementation in 2020.
(1) ADHD is now in the chapter Neurodevelopmental Disorders, which includes conditions associated with factors affecting the brain development.
(2) Diagnostic criteria have been adapted by adding some examples describing how ADHD symptoms are expressed across the lifespan.
(3) The age of onset criteria has been changed requiring several symptoms to be present before age of 12 years, instead of some symptoms and impairment by age 7.
(4) The term “subtype” has been replaced by “presentation”, reflecting the variation of ADHD symptoms within the same individual during the lifespan.
(5) The symptom threshold required has been reduced to 5 symptoms instead of six for older adolescents and adults (>17 years) in either the inattention or hyperactive/impulsive domain.
(6) Criteria requiring significant impairment has been modified to “clear evidence that symptoms interfere with or reduce the quality of social, academic and occupational functioning”, with specifiers regarding severity level.
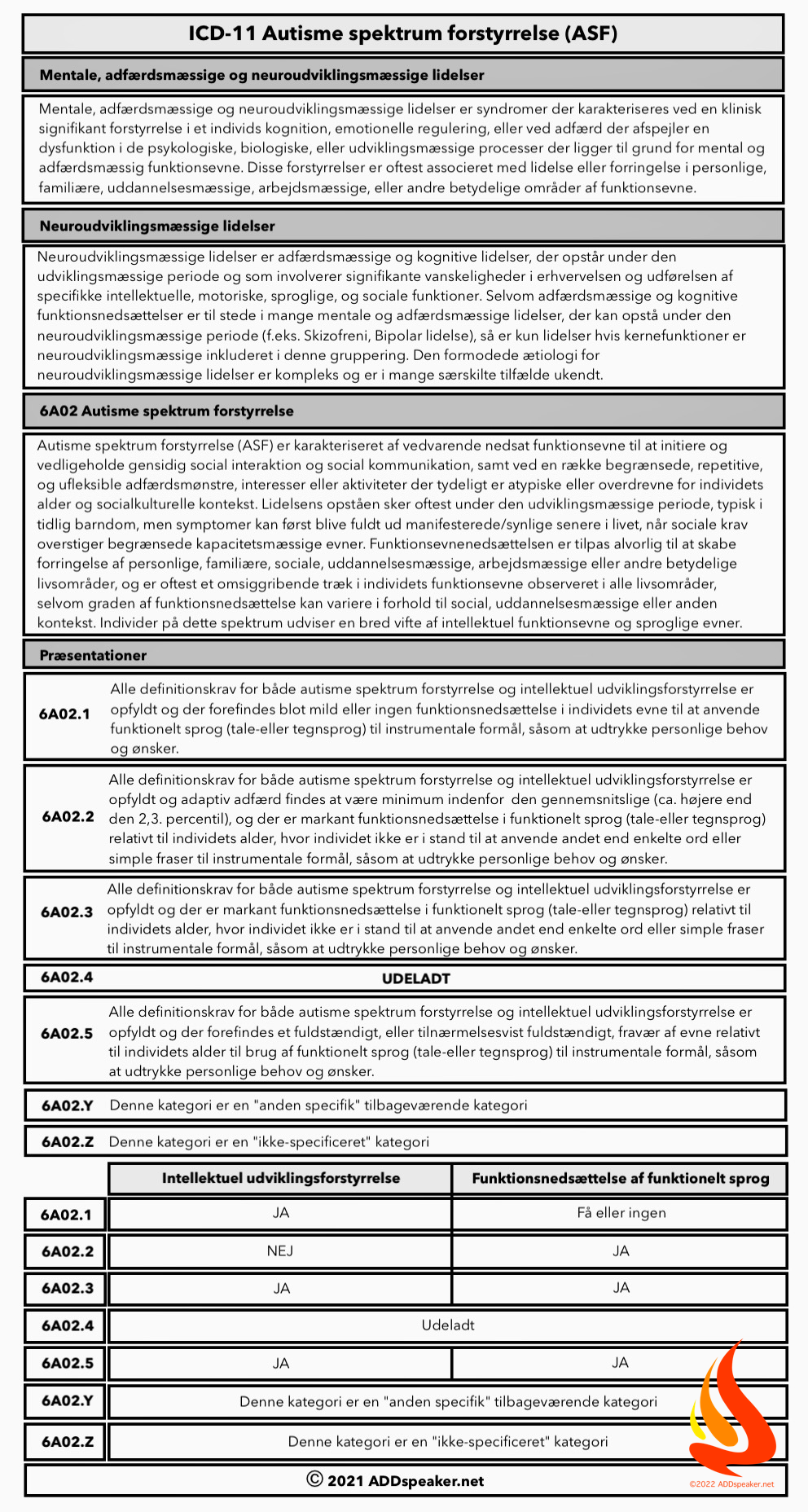
(7) The presence of Autism Spectrum Disorder (ASD) is no longer an exclusion criterion, consistent with evidence showing their frequent co-occurrence.
(8) ADHD Not Otherwise Specified (NOS) has been changed into Other Specified ADHD and Unspecified ADHD.
The revision of ICD-10, ICD-11 has been published in June 2018. ICD-11, developed by the World Health Organization now refers to ADHD as Attention Deficit Hyperactivity Disorder, instead of previously Hyperkinetic Disorder (HKD) [97]. It now uses similar requirements as the DSM-5 regarding age of onset, and the same 3 presentation types. In Europe, ICD codes are often used for statistics on mortality, morbidity and by insurance agencies for health-related reimbursements [98], whereas DSM is primarily used in clinical practice by licensed mental health care professionals [99]. (Kooij et al., 2019)
These changes recognise that impairment from the symptoms of ADHD may develop later in life and that in some cases symptoms cannot be clearly identified until the early adolescent years.
(Kooij et al., 2010)
Key changes in understanding of core symptoms of Adult ADHD have been put forward in the Updated European Consensus Statement on diagnosis and treatment of adult ADHD (Kooij et al., 2019). Here is a description of the key points.
Inattention and hyperfocus: Patients with mainly inattention problems are often slow to think and formulate due to distractions. They may formulate things in a long-winded and tangential way, losing themselves in irrelevant details and having difficulty making decisions. A difficulty for the clinician is that this may hinder the diagnostic assessment. Patients may also over-concentrate or ‘hyperfocus’. This phenomenon most commonly occurs when engaged in activities that the patient finds very interesting and/or provide instant gratification, such as computer games or online chatting. For such activities, concentration may last for hours on end, in a very focused manner (Kooij et al., 2019).
Hyperactivity: With respect to hyperactivity, adults do not present in the same way as children. Their hyperactivity usually manifests in a more subtle way. Clinicians need to assess their feelingsof restlessness. A first impression of mobility is not definitive; sitting calmly during the diagnostic assessment does not exclude any ADHD. Hyperactivity in adults often manifests itself as feelings of continuous inner restlessness or agitation, talking too much, ceaseless mental activity, not being able to relax properly or needing alcohol or drugs to relax and/or sleep. Hyperactivity and/or restlessness may be temporarily relieved by the patient engaging in excessive sport activities, and in such cases the person may suffer physical ailments as the body may have insufficient time to recover and/or due to sustained injuries (Kooij et al., 2019).
Impulsivity: Impulsive behavior and associated interpersonal conflicts often have consequences for relationships with family, friends, colleagues and employers. It may also seriously impact on personal finance when impulsive spending causes debt. Impulsive binge behaviors may also be present (e.g. binge eating), often to combat restlessness or due to a need for immediate gratification. Closely related to impulsivity are ‘sensation seeking’ behaviors when patients may seek out excitement from novel and thrilling stimuli. These often involve risk taking behaviors such as playing with fire, reckless driving, sexual risks, and provocative behavior leading to fights (Kooij et al., 2019).
Emotional dysregulation: Emotional dysregulation is listed by DSM-5 as a characteristic feature of ADHD, supporting the diagnosis [113]. The type of emotional dysregulation seen in ADHD has been characterized as deficient self-regulation of emotional symptoms such as irritability, frustration and anger [114], and low frustration tolerance, temper outbursts, emotional impulsivity, and mood lability [115]. Emotional dysregulation in ADHD is different from episodic symptoms such as marked sustained irritability occurring within the context of altered mood states, such as an episode of depression or mania. In ADHD, emotional symptoms tend to reflect short lived exaggerated changes, often in response to daily events, with rapid return to baseline within a few hours [114]. Whether the type of emotional instability seen in ADHD is qualitatively different to that seen in other chronic conditions such as borderline personality disorder or post-traumatic stress remains unclear (Kooij et al., 2019).
Excessive mind wandering: Another common feature of adult ADHD is excessive mind wandering, also referred to as mental restlessness [[116], [117], [118]]. In DSM-5 mind wandering is briefly mentioned as the occurrence of unrelated thoughts. Although mind wandering is a universal experience, some forms of mind wandering are detrimental because they interfere with task performance. Adults with ADHD frequently report a distractible mental state with multiple unrelated thoughts that are constantly on the go and jump from one topic to another [119,120]. Mind wandering is also a feature of other mental health disorders such as depressive or obsessive disorders. However, in ADHD mind wandering is characterized by unfocused, short lived distractible thoughts with no pattern of repeated thoughts or abnormality of content. Research found that excessive mind wandering was strongly correlated with ADHD symptoms, was a strong predictor of the diagnosis (sensitivity and specificity around 90% for case-control differences), co-varied with ADHD symptoms over a 6-month period, and was a better predictor of ADHD-related impairments than the inattentive and hyperactive-impulsive symptoms of ADHD [120]. In ADHD it can be measured using the Mind Excessively Wandering Scale [116,118,120] (Table 1) (Kooij et al., 2019).
Behavioral self-regulation (executive function deficits): ADHD has been described as a disorder of executive functions such as inhibition and working memory. These include problems organizing, prioritizing and initiating work; focusing, sustaining and shifting attention to tasks; regulating alertness, sustaining effort and processing speed; managing frustration and regulating emotions; utilizing working memory and accessing recall; and monitoring and self-regulation of behavior [121,122]. Although clinically these are good descriptions of the types of difficulties experienced by adults with ADHD, behavioral measures do not correlate well with cognitive or neuropsychological testsof executive control [[121], [122], [123]]. A distinction needs to be made between rating scalemeasures of behaviours reflecting self-regulation of behavior referred to as EF (behavioral) deficits, and the results of neurocognitive tests of EFs such as working memory and inhibition. Neuropsychological test scores reflecting executive functioning lack ecological validity in that they have no significant relationship to behavioural rating scale measures of EF [124]. The EF test scores also are very poor at predicting impairment in a variety of domains of major life activities, compared to EF behavioural rating scales [125] (Kooij et al., 2019).
Burden of ADHD: The impairments associated with ADHD across the lifespan are impressive. ADHD is associated with learning difficulties, school dropout, underachievement at work [126], frequent job changes [127], chronic fatigue [128], financial problems, gambling and internet use [129,130], home and traffic accidents leading to increased mortality rates [[131], [132], [133]], relationship difficulties and intimate partner violence [134,135], early onset of addiction [136], teenage pregnancies and sexual transmitted diseases [137,138], a two-fold increased smoking rate [139], an increased number of suicide attempts and self-harm in adolescents [140,141], and increased criminality [142,143]. Moreover, physical disorders and ailments may become chronic due to forgetfulness, health problems induced by a negative lifestyle, poor eating and sleeping habits, and lack of health care follow-up [[144], [145], [146], [147]]. ADHD has further been associated with auto-immune diseases [148], obesity [149], and physical multi-morbidity. In one large study, individuals with more than 4 diseases had over more than 3-fold higher odds of possible ADHD [146]. The risk of diabetes, hypertension, cardiovascular disease and cancer, that are related to obesity, may be increased as well. An additional burden on family life may be the presence of one or more children with ADHD, which happens frequently due to the high familial risks of the disorder (Kooij et al., 2019).
We therefore recommend that future criteria for ADHD are appropriately adjusted by taking into account age-related changes to symptoms and their relationship to impairment.
(Kooij et al., 2010)
Current evidence clearly defines ADHD as a clinical syndrome associated with impairments in multiple domains including academic difficulties, impaired family relationships, social difficulties and increased rates of conduct problems. In adults with ADHD increased rates of antisocial, drug use, mood and anxiety disorders are reported in both cross-sectional and longitudinal follow-up studies; in addition to increased rates of unemployment, poor work performance, lower educational performance, increased rates of traffic violations and accidents and criminal convictions: reviewed in NICE, [32] (Kooij et al., 2019).
Finally, the high familial risk among first degree relatives, in the order of 20% or more [20,194], means that a strong predictor for the ADHD in adults is having a parent, sibling or child with ADHD. Family history of ADHD should therefore raise the index of suspicion and provides further supportive evidence when evaluating individuals for ADHD (Kooij et al., 2019).
The treatment of adults with ADHD should follow a multimodal and multidisciplinary approach, which includes psychoeducation, pharmacotherapy, cognitive behavior therapy(CBT) and coaching for ADHD, which are all discussed in this article. Ideally, the treatment plan also involves the adult’s partner, family or close relationships, and in some cases systemic (family) therapy may be required when gross disruption to family relationships and functioning is present (Kooij et al., 2019).
In the most recent report of 20 nationally or regionally representative World Mental Health surveys, data on ADHD and comorbidities was collected on 26,744 respondents [202]. In adults with ADHD having one comorbidity was found in 23% of cases, two in 14% of case and three in 14% of cases. Rates were particulary high for any mood disorder (22%), any anxiety disorder (34%), substance use disorders (11%) and any behavioural disorder (15%). Treatment of ADHD is therefore most often in the context of co-occuring disorders (Kooij et al., 2019).
Before treatment starts, all comorbidities must be established so that the best order of treatment can be determined together with the patient. In general, the most severe disorder is prioritized. For instance, psychosis, bipolar disorder, substance abuse, severe depression and severe anxiety are usually treated first. Milder mood or anxiety disorders, and emotional instability, may respond to treatment of ADHD and can be treated at the same time as ADHD. Drug and alcohol abuse should be stabilized but can be treated at the same time as ADHD (Kooij et al., 2019).
According to consensus based on good clinical practice and the need to work on an informed consent basis within a multimodal treatment approach, psychoeducation should be the first step as a standard of care [217]. First evidence from an open trial and a randomized clinical trial shows, that patients and significant others who attend a structured psychoeducation program increase their knowledge about ADHD, and improve the quality of their relationships and psychological well-being [218,219] (Kooij et al., 2019).
In the first European Consensus Statement [1] psychostimulants (methylphenidate and dexamphetamine) were recommended as the first-line pharmacotherapy for adult ADHD [1,184,220], as they exert moderate-to-high clinical effects, with average effects higher than atomoxetine (ATX) and other non-stimulant medications [2]. There were, however, no head-to-head studies providing robust comparative analysis of efficacy differences [221]. Across most of Europe, lisdexamfetamine (LDX) has been introduced as a slow release formulation of dexamphetamine. The recent systematic review and network meta-analysis on the comparative efficacy and tolerability of medications for ADHD in children, adolescents and adults by Sam Cortese et al. showed, that the first pharmacological choice for ADHD in children and adolescents is methylphenidate, and amphetamines in adults [222]. In fact in adults, amphetamines were not only the most efficacious compounds, as rated by clinicians and by self-report, but also as well tolerated as methylphenidate and the only compounds with better acceptability than placebo (Kooij et al., 2019).
EFFICACY: Meta-analyses of randomized controlled trials (RCTs) demonstrate the efficacy of stimulants and ATX in the reduction of ADHD symptoms in adults [[223], [224], [225], [226], [227]]. Standardized mean differences (SMDs) range from 0.4 to 0.7, with stimulants showing greater efficacy than ATX [224]. The longest RCT in adults still found significant effects of MPH after one year [228]. National registry data also suggest long term benefits. Although these studies are not definitive due to lack of randomization and controls, they demonstrate ‘real-world’ societal benefits associated with the use of ADHD medications. These studies show that during periods of receiving medications for ADHD there are marked reductions in transport accidents and mortality rates [132,229], criminal convictions [230], suicidal behavior [231], violent reoffending [230], depression [232] and substance misuse [233]. Similar analyses with antidepressants find no effects, suggesting the effects are specific to ADHD medications (Kooij et al., 2019).
ADVERSE EFFECTS: The main adverse effects of stimulants are increased heart rate and blood pressure, and reduced appetite and sleep [[242], [243], [244], [245]]. Heart rate, blood pressure, sleep problems and weight are therefore assessed before, and monitored at least twice a year during treatment. Serious cardiac complications are rare [243,246,247] with reported risks for myocardial infarction, sudden cardiac death, ventricular arrhythmias or stroke no more than 0.2-0.4% higher in one study [248]. MPH might trigger arrhythmias in patients with congenital heart diseases [249]. The consensus is caution in patients with known cardiac defects, but risks are small (Kooij et al., 2019).
Currently there is no evidence of significant long-term risks using stimulants. Tomography scans find higher striatal dopamine transporter availability in ADHD patients treated with stimulants [271]. The clinical implications of this up-regulation are not clear. Potential toxicity on heart valves of medications with an agonist effect on 5-HT2B receptors have been discussed [272], including MPH and guanfacine. Some argue that echocardiography should be routinely performed prior to treatment with potential valvulopathic drugs [273]. This risk is not however established, and we and others do not recommend routine echocardiograms [184,252,274], except in older adults (> age 50) [167] (Kooij et al., 2019).
Because of the broad impact of ADHD on general functioning, the disorder is likely to have serious economic implications for children, families, and society. The studies which calculate costs however are so far limited as they typically examine only one aspect of the costs, for example “from the perspective of a major German health insurance fund” [332]. Particularly for adults with ADHD, estimates should include not only direct costs (the costs of labor, supplies, and equipment to provide direct patient care services) but also indirect costs (mainly related to the loss of productivity) such as costs to family, costs due to impairment in employment, costs due to accidents [333], smoking and substance misuse, and costs due to involvement with the criminal justice system (Kooij et al., 2019).
Direct costs have been examined [[334], [335], [336]], but are heavily depending on the healthcare system from which they are derived and the type of pathway/care package provided. These estimates therefore, although potentially useful for comparisons between disorders within the same healthcare system, should not be generalized to different contexts. The most comprehensive approach to calculate the total costs of ADHD in the Danish Psychiatric Central Register, showed that there is an economic burden of ADHD which is considerable and falls both on the individual and the state [337] (Kooij et al., 2019).
Apart from the costs (either direct or indirect) of ADHD, there is also the question of cost benefit for treating ADHD. This first asks whether a treatment of a disorder is worthwhile when compared against alternatives in terms of allocation of healthcare funds, and second which ADHD intervention brings the most benefit at the lowest cost. For the former, an argument can be made that adult ADHD is a condition which is cost effective to treat from the societal perspective because of the efficacy and relatively low cost of the medicines used for its treatment [224,338]. For the latter, among children and adolescents with ADHD, there is consistent evidence [[339], [340], [341], [342], [343]] that pharmacotherapies are cost effective compared with no treatment or behavioral therapy [344]. Unfortunately there is insufficient research to conclude the same for adults with ADHD (Table 3) (Kooij et al., 2019).
A summary of the main conclusions is listed in Table1.1
ADHD persists in adults in the majority of subjects with significant psychosocial impairment and a high comorbidity rate leading to high levels of personal distress and a substantial economic burden for society if left unidentified and untreated (Kooij et al., 2019).
The lifetime persistence of symptoms and impairment of ADHD is the hallmark of this disorder in the majority of cases.
(Kooij et al., 2010)
Diagnosis should include extensive psychiatric work-up including a detailed account of the developmental history, both current and retrospective account of ADHD symptoms and impairment and associated co-morbidities, before starting treatment. To prevent underreporting of symptoms, external validation is desirable by collecting information from relevant informants. The panel recommends multimodal treatment, comprising of psychoeducation, pharmacotherapy, coaching and/or cognitive behavioural therapy; and ideally involving the adult patient’s partner, family or close friends. Diagnostic and treatment services for adult ADHD should be established throughout Europe (Kooij et al., 2019).
European research into adult ADHD should be further developed in order to provide a better understanding of the way that ADHD presents from childhood until old age, to differentiate ADHD from common comorbidities and to improve treatment options.
(Kooij et al., 2019).
Read the full text of the study, it is an excellent summation of what we currently know about ADHD in adults, based on empirical scientific evidence – AKA – The Truth About Adult ADHD …
Updated European Consensus Statement on diagnosis and treatment of adult ADHD
Kooij SJ, Bejerot S, Blackwell A, et al.
European Psychiatry, Volume 56, 2019, Pages 14-34, ISSN 0924-9338,
https://doi.org/10.1016/j.eurpsy.2018.11.001
http://www.sciencedirect.com/science/article/pii/S0924933818301962
European consensus statement on diagnosis and treatment of adult ADHD: The European Network Adult ADHD
Sandra JJ Kooij, Susanne Bejerot, Andrew Blackwell, Herve Caci, Miquel Casas-Brugué, Pieter J Carpentier, Dan Edvinsson, John Fayyad, Karin Foeken, Michael Fitzgerald, Veronique Gaillac, Ylva Ginsberg, Chantal Henry, Johanna Krause, Michael B Lensing, Iris Manor, Helmut Niederhofer, Carlos Nunes-Filipe, Martin D Ohlmeier, Pierre Oswald, Stefano Pallanti, Artemios Pehlivanidis, Josep A Ramos-Quiroga, Maria Rastam, Doris Ryffel-Rawak, Steven Stes, Philip Asherson
BMC Psychiatry. 2010; 10: 67.
Published online 2010 Sep 3.
doi: 10.1186/1471-244X-10-67
PMCID: PMC2942810
This website uses cookies.

Tilføj din kommentar her - Feedback er altid velkomment!